It is particularly appropriate for Oregon to turn to the health care industry to fill a looming budget hole in its Medicaid program, the Oregon Health Plan. A pillar of the state’s health care system, the Oregon Health Plan insures over one million Oregonians. Unfortunately, Oregon’s Medicaid program faces a budget shortfall, in part due to a reduction in federal funds.
The Affordable Care Act, including its expansion of Medicaid, has benefitted much of the health care industry. So, it is fitting that the health care industry chip in more to support Oregon’s Medicaid program, allowing Oregonians to continue to receive the health care they need.
Read the executive summary of this report
Medicaid: A pillar of Oregon’s health care system
It is up to states to decide whether to run a Medicaid program. Under the program, states work within broad federal guidelines to provide health insurance to certain residents with modest incomes. The federal government reimburses states for much of the cost.
Oregon’s Medicaid program, the Oregon Health Plan (OHP), provides health insurance to over one million Oregonians — more than one in four residents. Medicaid plays a particularly vital role for Oregon children: Nearly 42 percent of Oregonians under age 19 are insured by OHP.[1]
Oregon’s expansion of the Oregon Health Plan in 2014, encouraged by the Affordable Care Act, has been the key driver in the sharp increase in the portion of Oregonians with health insurance. Oregon’s insured rate jumped from 85.3 percent in 2013 to 93.0 percent in 2015, largely due to OHP’s coverage of hundreds of thousands of additional Oregonians.[2]
Medicaid is great for Oregon’s economy
Medicaid is a great deal for Oregon. When Oregon invests in Medicaid, it triggers an investment by the federal government, pumping billions of federal dollars into the state’s economy.
How much a state receives from the federal government depends on a state’s economic circumstances and the number of people who sign up.[3] Oregon’s federal Medicaid “match” for 2017 is about 64 percent.[4] That means for every dollar Oregon spends in the Oregon Health Plan, the federal agency puts in $1.81 — a big bang for the state buck.
In some cases, the federal government contributes even more. The federal health agency pays for nearly all the costs for insuring certain groups of children.[5] Also, under the Affordable Care Act, the federal government currently pays 100 percent of the cost of insuring the 400,000 Oregonians added to Oregon’s Medicaid program as a result of the Act.[6] In 2017, the federal contribution for this expansion group will begin slowly phasing down, reaching 90 percent in 2020, where, under current law, it will remain. That means, in 2020, for every dollar Oregon spends on the Oregon Health Plan for that population, the federal government will chip in $9.
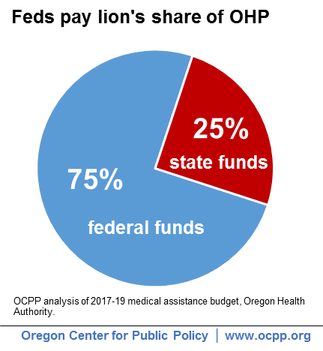
Overall, the federal government pays for the lion’s share of the Oregon Health Plan budget. In the 2017-19 budget period, federal funds are expected to cover about 75 percent of OHP, while Oregon contributes the remaining 25 percent.
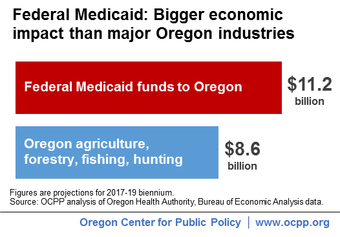
Medicaid not only protects the health of Oregonians, it also boosts the economy by bringing in billions in federal dollars. In the upcoming budget period, federal Medicaid payments will pump about $11.2 billion into Oregon — dollars that will flow to communities throughout the state.[7] For perspective, federal Medicaid spending in Oregon in 2017-19 will be more than the economic output of Oregon’s agricultural, forestry, fishing and hunting industries over the same period.[8]
Oregonians and the health industry contribute to the Oregon Health Plan
Where does the money for Oregon’s one-quarter share of this pillar of the state’s health care system come from?
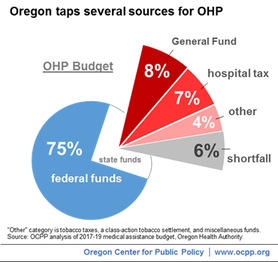
At present, Oregon taxpayers are the single largest source of state funds for OHP. About 8 percent of the OHP budget comes from the General Fund, which primarily consists of state income taxes paid by Oregonians. Current estimates show that the General Fund is expected to contribute about $1.1 billion to OHP in the 2017-19 budget period.[9]
The second largest source of the state’s Medicaid share – about 7 percent of the OHP budget – is a 5.3 percent tax on hospital net patient revenue.[10] This tax on hospitals — known as a health care provider tax — is expected to bring in about $1 billion in the 2017-19 biennium.[11]
The remainder of the budget comes from smaller sources of revenue, which include tobacco taxes, tobacco settlement funds, and other funds.[12] Resources for about 6 percent of the OHP budget are not yet identified and represent a budget shortfall.
The Oregon Health Plan faces a budget shortfall
The Oregon Health Plan faces a funding shortfall of $882 million in the upcoming 2017-19 budget period.[13]
About half of the budget gap is due to the fact that, starting in 2017, the federal government will no longer pay the full cost of the Medicaid expansion. In the 2017-19 biennium, the federal government will pay 94 percent of the cost of covering the new group.[14] Even then, Oregon will still be getting a great deal for insuring hundreds of thousands of residents, and the state will need to find a way to pay for its relatively small share of the costs.
Another driver of the budget gap is medical inflation. Oregon is breaking ground in controlling what otherwise might be runaway health care costs by instituting innovative health care coordination. Nevertheless, program costs rise by 3.4 percent per enrollee per year.[15]
Yet another cause of Oregon’s Medicaid funding gap is the expiration of federal funds that have supported Oregon’s innovative efforts to coordinate care and lower overall program costs.[16] In the absence of these funds, Oregon will need to invest in these efforts with its own dollars. While undoubtedly this will be money well-spent — since coordinated care and healthier enrollees can have large budgetary payoffs — it is a factor in the shortfall.
Unless Oregon finds a way to fill the budget gap, many Oregonians will lose health benefits or access to doctors — or both — and the state will lose nearly $1.5 billion in federal match dollars.
Keeping all Oregonians healthy requires additional resources
All Oregonians deserve a chance to be healthy, and yet many in our state lack access to adequate health services. Some 280,000 Oregonians, including many children, lack health insurance.[17] This is due to the fact that health insurance is still too expensive for many, as well as that our health care system still excludes some state residents because of their immigration status.[18]
Having health insurance, moreover, is no guarantee of getting necessary care. Oregonians with health insurance can find that essential health services are out of reach due to cost, inadequate coverage, discrimination, limited providers, and other barriers to care.[19]
Beyond filling the present funding gap, Oregon must invest more to ensure that all Oregonians can get the health care they need. Doing so would improve the health, quality of life, and economic potential of the state’s residents and the communities they live in.
Oregon should enact provider taxes to fill the Medicaid budget hole
Oregon should cover its Medicaid budget gap by increasing and establishing additional health care provider taxes. Specifically, lawmakers should increase the existing tax on hospital revenues, reinstate a tax on managed care organizations, and consider new taxes on other types of health care providers.
Looking to health care providers to fill the Medicaid budget gap is appropriate, given that the Affordable Care Act, and the Medicaid expansion in particular, have proved to be a boon for much of the health care industry. For example, net patient revenues at Oregon hospitals jumped 7.6 percent and 8.1 percent in 2014 and 2015, respectively, since the time major federal reforms came into effect.[20] By contrast, in the two years prior to reform, annual hospital net patient revenue increased about 2 percent or less.[21]
At the same time that hospitals have seen a sharp increase in revenues, their charity care outlays have plummeted because many more Oregonians are able to pay for hospital care through newly-acquired insurance. In 2013, prior to major reforms, Oregon hospitals provided $842 million in charity care. By 2015, that number dropped to $340 million — a 60 percent decline.[22]
Charity care is a justification for the non-profit status of Oregon hospitals. Nearly all Oregon hospitals are non-profits, and as such are exempt from business income taxes and property taxes. However, even as revenue has climbed and charity care has shrunk, Oregon non-profit hospitals continue to pay no business income taxes or property taxes.
Providers themselves can benefit from the Medicaid taxes they pay. Some of the tax dollars may return to them by virtue of the generous federal match and resulting increased Medicaid spending by the state, much of it going to pay for their services to the insured.
When used to fund Medicaid, state provider taxes need to be properly designed. While there is no limit on how much a state can raise from all providers (see Appendix A), the federal government has guidelines for how states structure provider taxes so that the revenues will qualify for the federal matching funds (see Appendix B).
In accordance with those guidelines, Oregon should:
Increase the current tax on hospital revenues
As mentioned above, Oregon hospitals have benefited handsomely from federal health reform.[23] Accordingly, the legislature should raise a significant portion of the Medicaid budget goal by increasing the state’s tax on hospitals. The American Hospital Association itself recognizes the importance of provider taxes in financing Medicaid.[24]
Oregon hospitals have contributed more to OHP than they do now. As of October 2014, the hospital tax was 5.8 percent, a level that was lowered to the current 5.3 percent rate effective April 2016, when the state determined it did not need the higher revenues at that time.[25]
Governor Brown has proposed increasing the state’s tax on hospitals, with the details of the proposal reportedly still to be worked out.[26] Her budget proposes biennial revenues from a revised tax on hospitals at $379 million, as shown in Table 1.[27]
Reinstate a tax on managed care organizations
Another option for helping to fill the Medicaid budget gap is reestablishing a tax on managed care organizations, a proposal also included in Governor Brown’s 2017-19 budget. While Oregon currently has two types of provider taxes — on hospitals and nursing facilities — most states use three or more types of provider taxes to pay for their Medicaid programs (see Appendix C).
Indeed, in the past, Oregon had a third provider tax. A tax on Medicaid managed care organizations helped to pay for health insurance for Oregon children from 2009 to 2013. During that time period, Oregon levied a 1 percent tax on the payments that Medicaid managed care companies received from the state to serve OHP enrollees. The tax was estimated to generate $40.1 million in 2011-13.[29]
While the details of the Governor’s proposed tax on managed care organizations are reportedly yet to be determined, this is a revenue source the Oregon legislature ought to pursue.
Consider new taxes on other health care providers
Oregon should consider other sources of revenue from providers to avoid program cuts and protect this pillar of Oregon’s health care system. Indeed, other health care providers financially benefit from the state’s expanded Medicaid program.
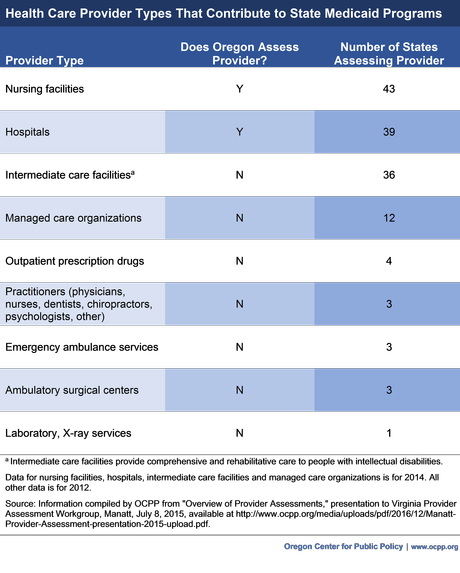
According to federal guidance, revenue generated from a variety of health care provider types may qualify for federal Medicaid match. These provider types include intermediate care facilities (which provide comprehensive and rehabilitative services to people with intellectual disabilities), physicians, nurses, dentists, chiropractors, psychologists, emergency ambulance services, ambulatory surgical centers, and free-standing laboratory and X-ray services. Outpatient prescription drugs may also be taxed.[30]
Oregon would be in good company in turning to these providers to help finance the state’s share of Medicaid. Many states ask these types of practitioners to contribute to operating their Medicaid programs (see Appendix C).
Oregon can also tap other health industry players to fill the Medicaid budget gap
States can raise funds for Medicaid from non-providers in the health industry without federal restriction. Some states finance Medicaid through taxes on health insurance premiums and health insurance claims. Unlike taxes on Medicaid managed care payments, these kinds of taxes are not considered provider taxes by the federal government and, therefore, do not need to conform to federal rules governing provider taxes.[31]
Together with the Medicaid managed care tax, Oregon has imposed a tax on insurers in the past to pay for children’s health insurance. From 2009 to 2013, Oregon levied a 1 percent tax on health insurance premiums in Oregon, including premiums of Oregon’s Public Employees Benefit Board (PEBB) health plans. The taxes generated an estimated $129.5 million in 2011-13, as shown in Table 1.[32]
In her 2017-19 budget, Governor Brown proposes to levy a tax on health insurance premiums. Her published budget does not clarify whether it applies to PEBB plans. With the tax on managed care organizations described in the section above, the proposed premium taxes are expected to generate $151 million over the biennium, as shown in Table 1.[33]
Official estimates of revenues from a health insurance claims tax in Oregon are not available as of this writing. Table 1 includes figures for a Michigan tax of this type and an estimate of the level of biennial revenues that might be generated in Oregon — $252.1 million — should the state choose to institute such a tax. 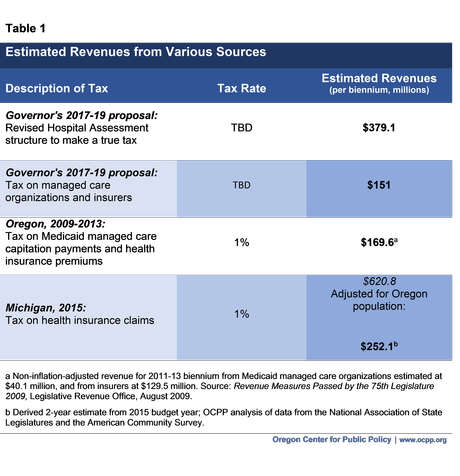
Conclusion
Medicaid is a critical part of Oregon’s social infrastructure. Through the Oregon Health Plan, it provides health insurance to one in four Oregonians, nearly all of whom would otherwise go without coverage and struggle to get preventive and other needed care. The health care industry has benefitted greatly from the Affordable Care Act’s expansion of Medicaid. Accordingly, it makes sense to look to the health care industry to address OHP’s funding needs.
Appendix A: No federal limit on total provider taxes
There is no limit on the total amount that a state can raise from provider taxes to pay for the state’s share of Medicaid costs.
There has been some confusion on this issue, owing to language in a federal statute that has expired. That statute contained a provision limiting the amount a state could raise through provider taxes to 25 percent of a state’s total contribution. A subsequent statute, however, sunset the limitation as of 1995. Congress has not reinstated the limit since.
An example of this confusion appeared in a document on program financing by the Medicaid and CHIP Payment and Access Commission (MACPAC), Congress’s independent policy analysis office. While the document initially the claimed that there is a 25 percent limit, the commission later issued a correction, recognizing the error:
Erratum: Please note that the statement on p. 175, “The amount of Medicaid funding that may be generated through health-care related taxes generally cannot exceed 25 percent of the total non-federal share in a given year” was in error. This was a time-limited provision in statute that has since expired.[34]
Appendix B: Federal guidelines for provider taxes
Federal guidelines specify how states can structure a tax on health providers to generate revenue that will qualify for the federal match. According to the guidelines, the tax must meet several tests:[35]
-
- Broad-based. The tax must be levied on all providers within a specified class of providers, not just providers that serve Medicaid recipients. Federal law specifies 19 classes of providers used to ensure this standard. These include services of inpatient hospitals, outpatient hospitals, nursing facilities, intermediate care facilities for people with intellectual disabilities, physicians, home health care providers, managed care organizations, ambulatory surgical centers, dental centers, podiatrists, chiropractors, optometrists, opticians. They also include psychological services, therapist services, nursing services, laboratory and X-ray services provided at free-standing facilities, and outpatient prescription drugs.
-
-
- Uniform.The tax must be the same rate for all providers within the class
-
-
-
-
- No hold harmless effect. States cannot provide a direct or indirect guarantee that providers will receive their money back through state reimbursements for providing Medicaid services. Several “tests” determine whether states offer a direct or indirect guarantee of repaying providers. The first is whether the tax is applied at a rate below 6 percent of net patient revenues. This threshold is known as a “safe harbor,” since if met, no other test regarding distributive impacts is needed. If the tax exceeds the safe harbor threshold, a second test must be met, namely that more than 75 percent of the taxed providers do not receive more than 75 percent of the revenues from the tax through higher Medicaid reimbursement rates. If a state violates the “75/75” rule, the revenues of the tax can still go to support the program but would not be eligible for federal match.
-
-
Federal officials are allowed to waive the broad-based and uniform requirements if a state can show that the net impact of the tax is “generally redistributive” and the amount of the tax is not directly related to Medicaid payments.
Oregon’s hospital tax is currently below the 6 percent safe harbor threshold, at 5.3 percent of net patient revenues. The federal threshold has been temporarily lowered to 5.5 percent in the past.[36]
Appendix C: Types of providers that fund state Medicaid programs
States currently use taxes on a range of health industry providers to finance their Medicaid programs. The following chart shows the recent incidence of various types of provider taxes, including in Oregon.
[1] OCPP analysis of Oregon Health Authority administrative data, October 15, 2016.
[2] OCPP analysis of American Community Survey data. Also, Governor’s Budget, 2017-19, p. 64, available at.
[3] The lower a state’s per capita income, the higher the Medicaid match rate.
[4] The federal Medicaid match rate for Oregon’s categorically eligible population for October 2016 – September 2017 is 64.47 percent. “FY2017 Federal Medical Assistance Percentages,” Office for the Assistant Secretary for Planning and Evaluation, U.S. Department of Health and Human Services, December 29, 2015.
[5] Oregon’s federal match rate for covering children under the Children’s Health Insurance Program (CHIP) — those above the Medicaid categorical eligibility level up to 300 percent of the federal poverty level — was temporarily boosted under the Affordable Care Act. For the 2017 federal fiscal year, Oregon’s federal match rate under CHIP is 98.13. Ibid.
[6] Governor’s Budget 2017-19, p. 64.
[7] [Untitled document], Oregon Health Authority, September 18, 2016.
[8] The Oregon agriculture, forestry, fishing and hunting industry is estimated at $8.6 billion in the 2017-19. OCPP analysis of Bureau of Economic Analysis data.
[9] Unless otherwise noted, all estimates of funding for the Oregon Health Plan for 2017-19 are from [untitled document], Oregon Health Authority, September 18, 2016.
[10] State of Oregon Tax Expenditure Report: 2017-19 Biennium, Oregon Department of Revenue, p. 391.
[11] Oregon assesses another provider tax on nursing facilities to take care of low-income Oregonians needing long-term nursing care. These costs are not included in the OHP budget.
[12] In addition to tobacco taxes and tobacco settlement funds, other smaller sources of revenue are drug rebates, settlements, other public entity money such as from counties, and any other money. Email communication with Jeston Black, Oregon Health Authority, December 6, 2016.
[13] Op. cit. ibid. [untitled document], Oregon Health Authority, September 18, 2016.
[14] Specifically, in the later part of 2017, the federal share of the Medicaid expansion population will be 95 percent of program costs, with Oregon picking up the other 5 percent. The federal government’s share will decrease to 94 percent in 2018 and further thereafter until it reaches 90 percent in 2020. See Rudowitz, Robin, Understanding How States Access Enhanced Federal Match Rate, Kaiser Family Foundation, p. 2.
[15] The medical rate of growth allowed under Oregon’s Medicaid contracts with Coordinated Care Organizations is 3.4 percent per person per year. Op. cit. ibid. [Untitled document], Oregon Health Authority, September 18, 2016.
[16] Federal Designated State Health Programs (DSHP) funds that Oregon has been receiving to pay for OHP services not typically allowed under Medicaid are no longer available starting in the 2017-19 biennium. Ibid. See Governor’s Budget 2017-19, p. 61.
[17] OCPP analysis of 2015 American Community Survey data.
[18] Mend the Gap: Why full coverage makes sense for Oregon, Oregon Health Equity Alliance, November 2015.
[19] Ibid.
[20] Net patient revenue is the amount a hospital bills for patient care after accounting for contractual allowances to third party payers and for uncompensated care.
[21] Oregon Acute Care Hospitals, Annual Financials Reporting Highlights 2015, Oregon Health Authority, presented July 25, 2016.
[22] Ibid.
[23] In addition to increased business demand and lower uncompensated care outlays, it is worth noting that nearly all Oregon hospitals receive some amount of federal “Disproportionate Share Hospital” (DSH) funds, intended for safety net hospitals that serve a disproportionate share of Medicaid patients and uninsured residents. (See annual state DSH reports available at https://www.medicaid.gov/medicaid/financing-and-reimbursement/dsh/). Although the Affordable Care scaled back DSH payments starting in 2014 due to fewer uninsured individuals, Congress has delayed the reductions several times. DSH reductions are now postponed until 2018. In 2015, Oregon received a federal DSH allotment of $49,047,232, according to preliminary government numbers. Federal Register, Nol. 81, No. 21, February 2, 2016, p. 5455.
[24] Medicaid Provider Assessments, fact sheet, American Hospital Association, August 2016.
[25] Oregon Bulletin, Oregon Secretary of State, May 1, 2016.
[26] Op. cit. ibid. Governor’s Budget 2017-19.
[27] Email communication with Jeston Black, Governmental Relations Director, Oregon Health Authority, December 9, 2016.
[28] Revenue Measures Passed by the 75th Legislature, Research Report #5-09, Legislative Revenue Office, August 2009.
[29] Email communication with Jeston Black, Governmental Relations Director, Oregon Health Authority, December 12, 2016.
[30] 42 CFR Ch. IV, 433.55.
[31] Medicaid Reforms to Expand Coverage, Control Costs and Improve Care: Results from a 50-State Medicaid Budget Survey for State Fiscal Years 2015 and 2016, Kaiser Family Foundation, October 2015, available at http://files.kff.org/attachment/report-medicaid-reforms-to-expand-coverage-control-costs-and-improve-care-results-from-a-50-state-medicaid-budget-survey-for-state-fiscal-years-2015-and-2016.
[32] Op. cit. ibid., Revenue Measures Passed by the 75th Legislature, Research Report #5-09, Legislative Revenue Office, August 2009.
[33] Email communication with Jeston Black, Governmental Relations Director, Oregon Health Authority, December 9, 2016.
[34] MACPAC is a non-partisan legislative branch agency that provides policy and data analysis and makes recommendations to Congress, the U.S. Department of Health and Human Services and others. State Financing of Medicaid: Context, Scope, and Relationship to Provider Payment, MACPAC, March 2012, available at https://www.macpac.gov/publication/ch-3-state-approaches-for-financing-medicaid-and-update-on-federal-financing-of-chip/.
[35] 42 C.F.R. 433.56. See also, Medicaid Provider Taxes, Congressional Research Service, March 15, 2012, pp. 4-5.
[36] Medicaid Financing: States’ Increased Reliance on Funds from Health Care Providers and Local Governments Warrants Improved CMS Data Collection, U.S. General Accounting Office, July 2014, p. 50.